
Understanding Benefit Verification: A Technical Breakdown of Its Failures and Constraints
Understanding Benefit Verification: A Technical Breakdown of Its Failures and Constraints
The problem
Benefit Verification (BV) remains one of healthcare’s most manual and costly workflows, despite decades of digitization. The 2024 CAQH Index estimates over $20 billion in annual savings still available if remaining manual BV steps were automated [1]. Nearly 90% of eligibility checks are now electronic, yet most of the work that actually determines access, coverage interpretation, cost-share calculation, and prior-authorization validation, still requires human effort [2].
Where this burden is rising fastest is exactly where automation struggles most: specialty medications.
In 2021, specialty drugs accounted for just 6.2% of prescriptions but 71.1% of total drug spending [3].By 2027, employers are projected to spend more than 56% of total drug costs on these therapies, despite representing a small minority of total prescriptions [4].
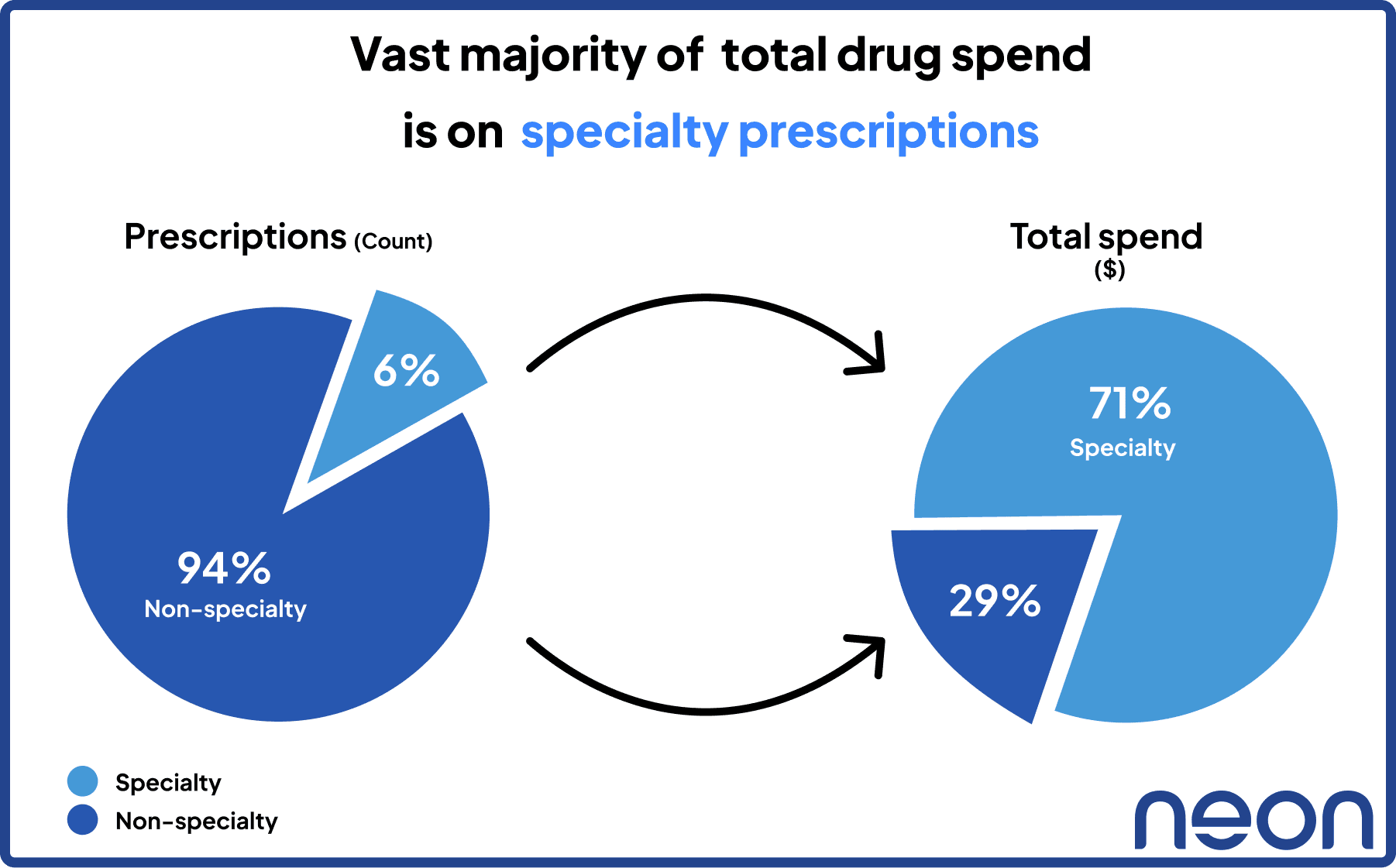
Figure 1: Share of prescriptions vs. share of spend (Speciality / Non-specialty)
The therapies that matter most clinically and financially are the hardest to verify operationally. Specialty therapies require multiple payer lookups, cross-portal checks, policy interpretation, site-of-care validation, and channel routing. Each case is materially harder than a standard eligibility check, and much harder to automate with today’s fragmented data infrastructure. That’s why BV has become the hidden bottleneck in modern patient access.
The question facing healthcare leaders today isn’t whether automation exists. It’s why, after all this progress, automation still cannot keep up with the complexity of real-world benefit verification.
The Anatomy of a Benefit Verification (BV)
A Benefit Verification is often described as “checking coverage,” but in practice, it is a multi-component data-gathering and interpretation workflow that spans eligibility, benefit design, access rules, financial responsibility, and documentation.
Most delays, rework, and errors in the access ecosystem originate because these components must be stitched together manually and interpreted in context, usually across multiple disconnected systems.
A complete BV typically includes four core stages.
Stage 1: Intake: Establishing the Case
This is where access teams collect the baseline information required to begin any verification:
Patient & plan identifiers
Payer/PBM
Member ID, group number
Referral details, diagnosis, and intended therapy
Planned site of service (for medical benefit)
Provider/facility NPI(s)
This step determines what kind of BV is required: pharmacy, medical, or dual-channel.
Stage 2: Eligibility & Coverage: Confirming Active Coverage
This is the only part of BV that is largely electronic today. EDI 270/271 transactions can return:
Active/inactive coverage
Product line (commercial, MA, Medicaid, exchange)
Basic copay/coinsurance benefits
Plan-level deductible and OOP max information
But these transactions do not return the therapy-specific information needed to determine whether a drug or service is actually covered, which is why this stage still relies heavily on payer portals, PDFs, and phone/IVR systems.
According to the 2024 CAQH Index, 89% of eligibility checks are now electronic, but the rest of BV remains overwhelmingly manual [2].
Stage 3: Cost Share & Requirements: Interpreting the Benefit
This is the most complex, and the most failure-prone part of BV. Teams must determine:
Prior authorization requirement
Step therapy or fail-first rules
Quantity limits and dosing restrictions
Channel routing (pharmacy vs medical)
Site-of-care constraints (hospital vs. physician office vs. home infusion)
Specialty network requirements
Estimated OOP after deductible, OOP max, and accumulators
Crucially, none of these rules are standardized electronically. They live in:
IVR trees
Payer/PBM portals
Medical policy PDFs
Prior authorization grids or Excel tables
Provider manuals
Specialty network lists
FAQ pages and plan brochures
This is why specialty medications, despite representing only 6.2% of prescriptions, require disproportionate effort and delay [3].
Stage 4: Documentation & Handoff: Producing the “Source of Truth”
Every BV must produce an audit-ready artifact that downstream teams can use:
Screenshots
Portal excerpts
Policy links or PDFs
IVR reference numbers
Manual notes capturing coverage confirmations
Structured fields entered into CRM, EHR, or a case system
Without proper documentation, BV results cannot be trusted by:
PA teams
Providers
Pharmacies
Payer audit teams
This is also where the most rework originates, because incomplete or missing documentation forces teams to redo the entire verification.
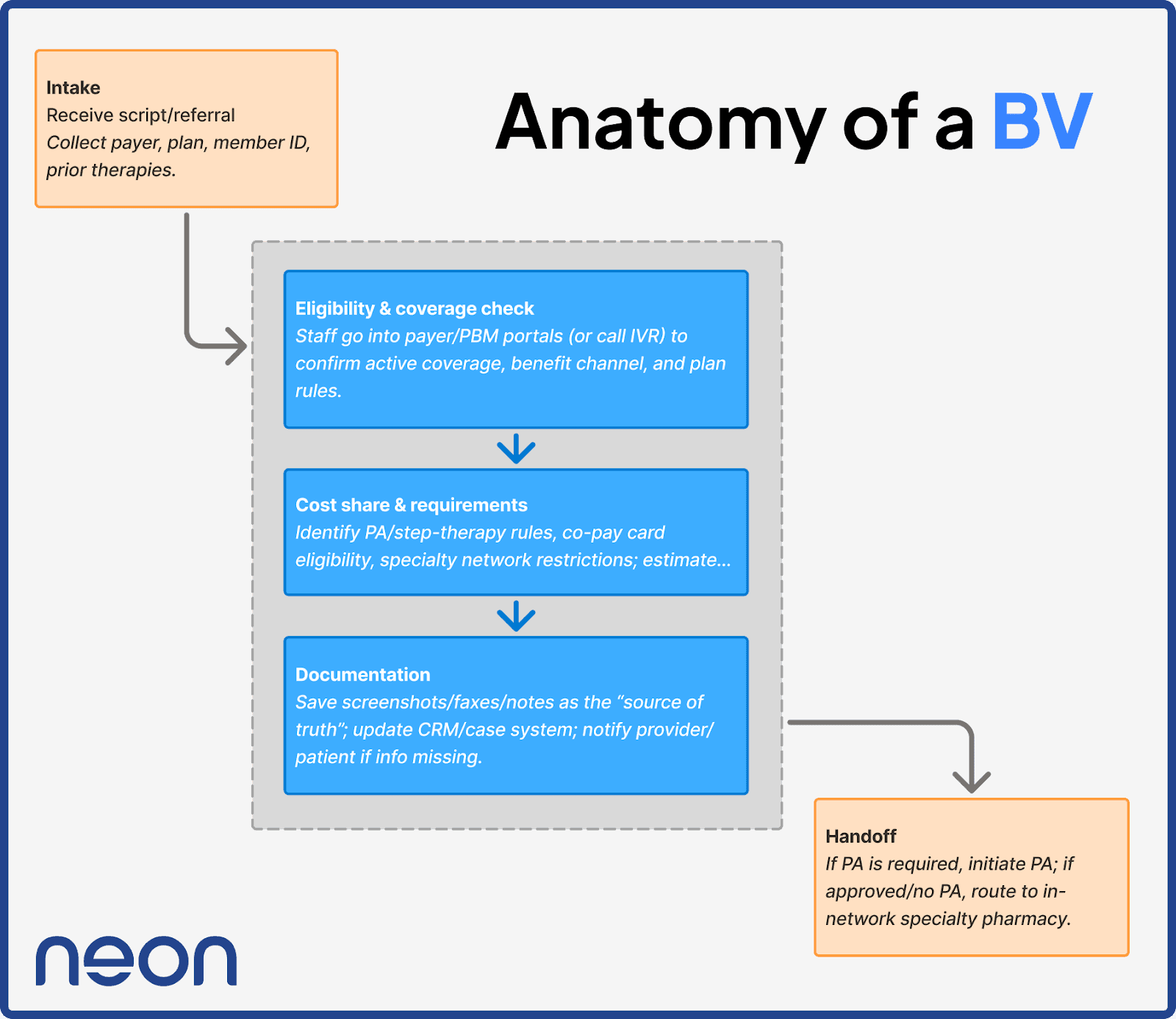
Figure 2: Anatomy of benefit verification
Why This Anatomy Matters
Each of these components introduces latency, fragmentation, and human interpretation. Together, they explain why:
Manual BV volume increased 38% year-over-year in 2024 [1]
“Partially electronic” BV is declining, because specialty workflows cannot be partially automated
Providers, hubs, and pharma teams spend tens of minutes per prescription and hours per day gathering data instead of moving patients forward
BV is not one task, it’s dozens of microtasks, stitched together manually, repeated thousands of times across the healthcare system. And that is exactly where the system breaks.
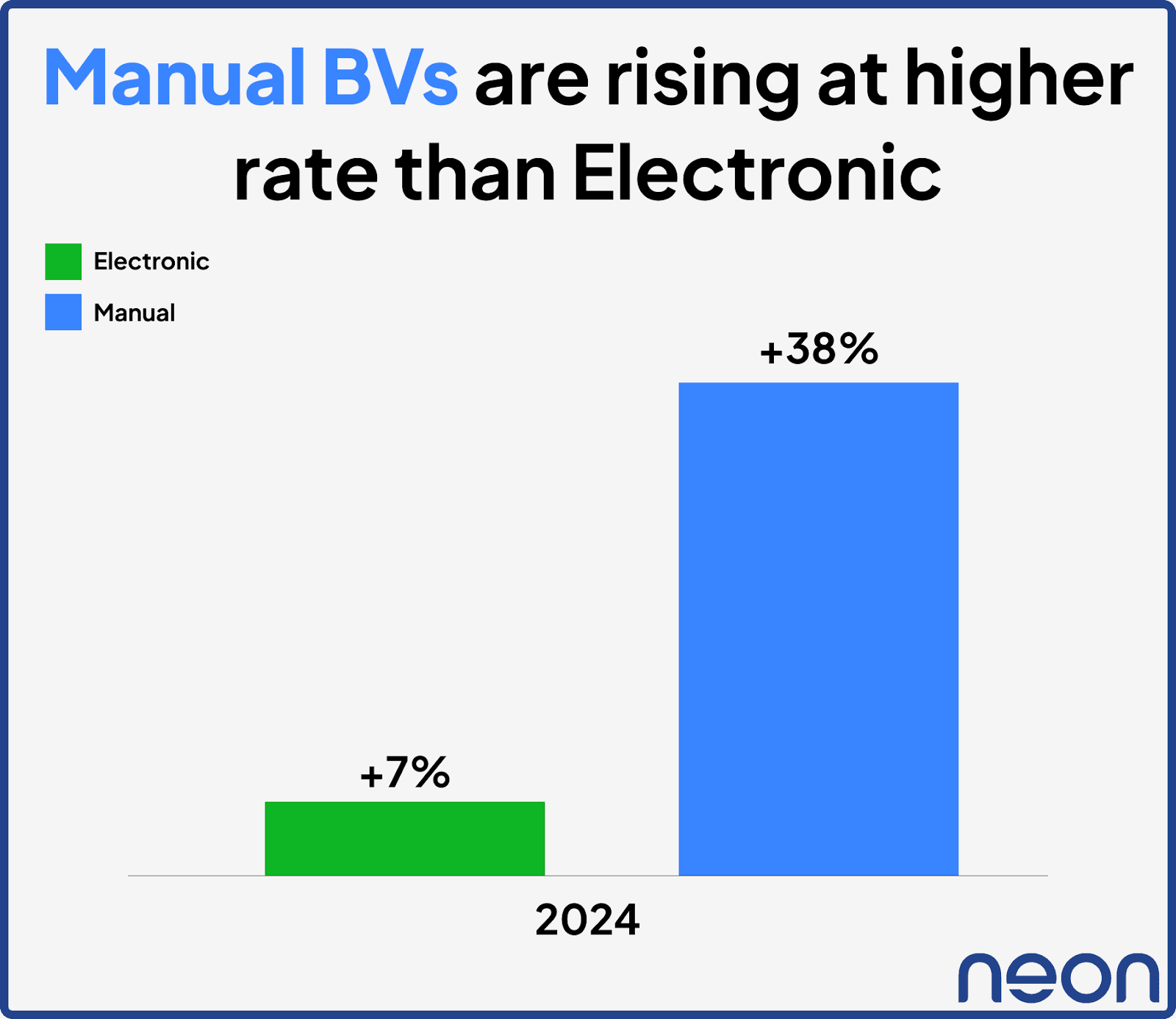
Figure 3: YoY % Rate of increase of BV volumes
Why Today’s BV Infrastructure Cannot Keep Up
The BV workflow for specialty prescriptions is clear: a sequence of disconnected tasks that rely heavily on human interpretation. The deeper question is why, after decades of digitization, these tasks still cannot be automated at scale. The root issue is structural.
Modern healthcare data standards were built to exchange coverage data. EDI 270/271 transactions accurately return active coverage status, product line, and basic financials, but they were never intended to express therapy-specific rules, prior authorization criteria, step therapy sequences, quantity limits, or specialty-pharmacy requirements. These rules generally don’t exist in machine-readable formats [1][2].
As therapies have grown more complex, this gap has widened. Specialty medications, only 6.2% of prescriptions but 71.1% of spending, require the deepest review, the most variations across payers, and the most documentation [3]. The BV infrastructure simply wasn’t designed for this level of variability.
Workflow design compounds the problem. Benefit Verifications still require sequential, IVR/portal-based work, one case, one portal, one policy, one screenshot at a time. There is no way to orchestrate multi-source checks in parallel or automatically synthesize evidence across portals, PDFs, IVR calls, and policy documents. As volume increases, particularly for specialty drugs, throughput hits a natural ceiling.
Finally, BV outputs are still largely unstructured: screenshots, pasted notes, or free-text fields. Downstream teams, PA coordinators, pharmacies, providers, cannot rely on these outputs programmatically, which means every step after BV inherits the same manual burden. Without structured, auditable outputs, no downstream automation can be triggered reliably.
In short, BV fails today because the system was designed to move data, not to understand it. Eligibility became electronic, but the logic that determines access never followed. The industry now faces a structural problem, not a workflow problem, and solving it requires an entirely different foundation.
Closing the Gap
The challenges in BV persist because the underlying infrastructure cannot express or interpret benefit logic. Eligibility data moves electronically, but the information required to determine access, prior authorization criteria, step therapy, quantity limits, specialty-network rules, and site-of-care restrictions, remains locked in formats designed for humans, not systems, in particular IVR trees.
Neon Health approaches the problem by focusing on the underlying data model rather than the workflow. The system is built to do three things reliably:
1. Retrieve information from the sources where benefit logic actually lives.
This includes payer and PBM portals, policy documents, and electronic transactions. The goal is not to replace these sources but to read and extract from them consistently.
2. Interpret and normalize benefit rules into a structured format.
Coverage policies vary widely by payer and plan. Neon translates this variation into a uniform schema so that prior authorization requirements, quantity limits, and cost-share details can be evaluated consistently.
3. Produce a complete, evidence-linked verification record.
Every value captured, coverage status, access requirements, financial information, is stored alongside its source. This creates a verifiable BV artifact that downstream teams can use without rework.
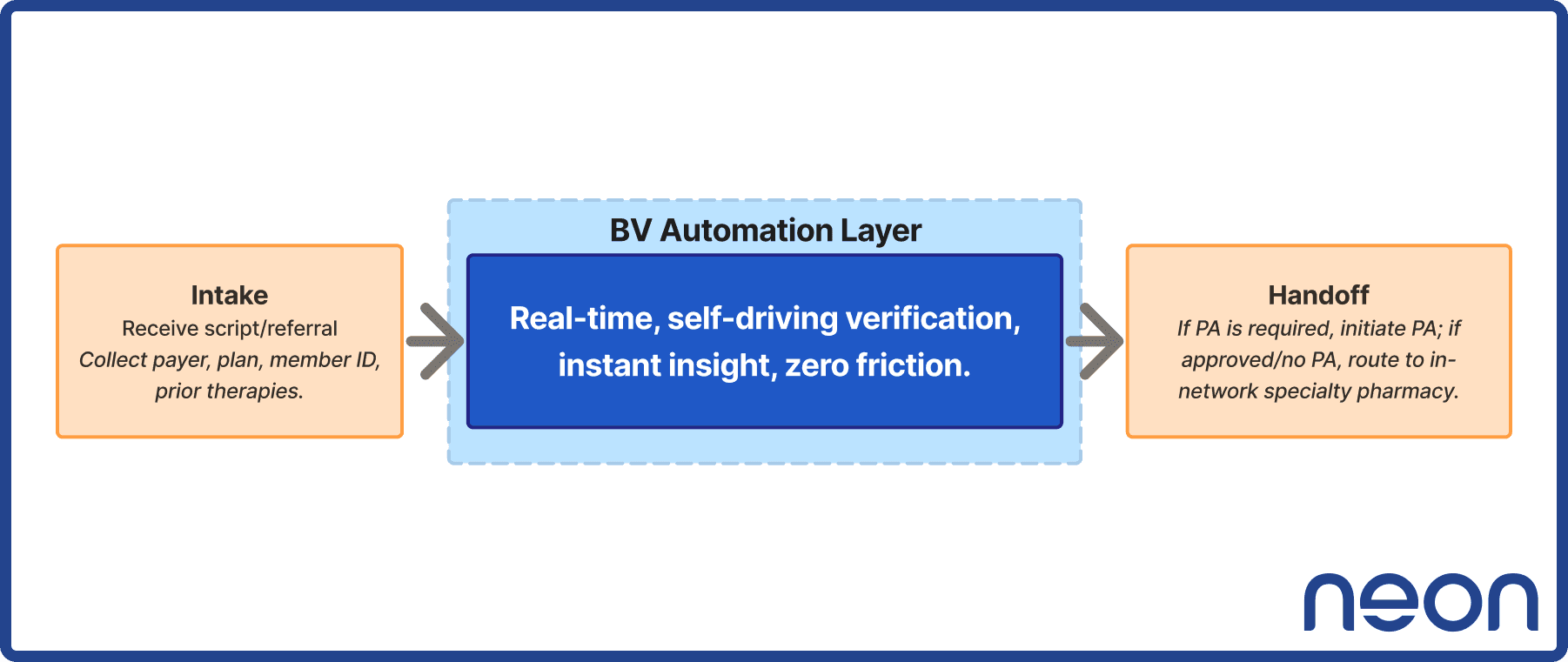
Figure 4: Neon Health BV Acceleration Layer
This does not eliminate the complexity of benefit design, nor does it replace clinical or operational judgment. It simply removes the manual steps required to retrieve, interpret, and document the information that determines access. By treating BV as a data standardization and interpretation problem, rather than a portal-navigation task, Neon provides an infrastructure that can scale with the volume and variability of today’s therapies.
The result is not a different workflow, it is a more reliable foundation for the same decisions access teams make every day.
Sources
[2] CAQH Index 2024 – Full Report (PDF)
[4] MedCity News (2024): Managing the Specialty Drug Cost Challenge
The problem
Benefit Verification (BV) remains one of healthcare’s most manual and costly workflows, despite decades of digitization. The 2024 CAQH Index estimates over $20 billion in annual savings still available if remaining manual BV steps were automated [1]. Nearly 90% of eligibility checks are now electronic, yet most of the work that actually determines access, coverage interpretation, cost-share calculation, and prior-authorization validation, still requires human effort [2].
Where this burden is rising fastest is exactly where automation struggles most: specialty medications.
In 2021, specialty drugs accounted for just 6.2% of prescriptions but 71.1% of total drug spending [3].By 2027, employers are projected to spend more than 56% of total drug costs on these therapies, despite representing a small minority of total prescriptions [4].
Figure 1: Share of prescriptions vs. share of spend (Speciality / Non-specialty)
The therapies that matter most clinically and financially are the hardest to verify operationally. Specialty therapies require multiple payer lookups, cross-portal checks, policy interpretation, site-of-care validation, and channel routing. Each case is materially harder than a standard eligibility check, and much harder to automate with today’s fragmented data infrastructure. That’s why BV has become the hidden bottleneck in modern patient access.
The question facing healthcare leaders today isn’t whether automation exists. It’s why, after all this progress, automation still cannot keep up with the complexity of real-world benefit verification.
The Anatomy of a Benefit Verification (BV)
A Benefit Verification is often described as “checking coverage,” but in practice, it is a multi-component data-gathering and interpretation workflow that spans eligibility, benefit design, access rules, financial responsibility, and documentation.
Most delays, rework, and errors in the access ecosystem originate because these components must be stitched together manually and interpreted in context, usually across multiple disconnected systems.
A complete BV typically includes four core stages.
Stage 1: Intake: Establishing the Case
This is where access teams collect the baseline information required to begin any verification:
Patient & plan identifiers
Payer/PBM
Member ID, group number
Referral details, diagnosis, and intended therapy
Planned site of service (for medical benefit)
Provider/facility NPI(s)
This step determines what kind of BV is required: pharmacy, medical, or dual-channel.
Stage 2: Eligibility & Coverage: Confirming Active Coverage
This is the only part of BV that is largely electronic today. EDI 270/271 transactions can return:
Active/inactive coverage
Product line (commercial, MA, Medicaid, exchange)
Basic copay/coinsurance benefits
Plan-level deductible and OOP max information
But these transactions do not return the therapy-specific information needed to determine whether a drug or service is actually covered, which is why this stage still relies heavily on payer portals, PDFs, and phone/IVR systems.
According to the 2024 CAQH Index, 89% of eligibility checks are now electronic, but the rest of BV remains overwhelmingly manual [2].
Stage 3: Cost Share & Requirements: Interpreting the Benefit
This is the most complex, and the most failure-prone part of BV. Teams must determine:
Prior authorization requirement
Step therapy or fail-first rules
Quantity limits and dosing restrictions
Channel routing (pharmacy vs medical)
Site-of-care constraints (hospital vs. physician office vs. home infusion)
Specialty network requirements
Estimated OOP after deductible, OOP max, and accumulators
Crucially, none of these rules are standardized electronically. They live in:
IVR trees
Payer/PBM portals
Medical policy PDFs
Prior authorization grids or Excel tables
Provider manuals
Specialty network lists
FAQ pages and plan brochures
This is why specialty medications, despite representing only 6.2% of prescriptions, require disproportionate effort and delay [3].
Stage 4: Documentation & Handoff: Producing the “Source of Truth”
Every BV must produce an audit-ready artifact that downstream teams can use:
Screenshots
Portal excerpts
Policy links or PDFs
IVR reference numbers
Manual notes capturing coverage confirmations
Structured fields entered into CRM, EHR, or a case system
Without proper documentation, BV results cannot be trusted by:
PA teams
Providers
Pharmacies
Payer audit teams
This is also where the most rework originates, because incomplete or missing documentation forces teams to redo the entire verification.
Figure 2: Anatomy of benefit verification
Why This Anatomy Matters
Each of these components introduces latency, fragmentation, and human interpretation. Together, they explain why:
Manual BV volume increased 38% year-over-year in 2024 [1]
“Partially electronic” BV is declining, because specialty workflows cannot be partially automated
Providers, hubs, and pharma teams spend tens of minutes per prescription and hours per day gathering data instead of moving patients forward
BV is not one task, it’s dozens of microtasks, stitched together manually, repeated thousands of times across the healthcare system. And that is exactly where the system breaks.
Figure 3: YoY % Rate of increase of BV volumes
Why Today’s BV Infrastructure Cannot Keep Up
The BV workflow for specialty prescriptions is clear: a sequence of disconnected tasks that rely heavily on human interpretation. The deeper question is why, after decades of digitization, these tasks still cannot be automated at scale. The root issue is structural.
Modern healthcare data standards were built to exchange coverage data. EDI 270/271 transactions accurately return active coverage status, product line, and basic financials, but they were never intended to express therapy-specific rules, prior authorization criteria, step therapy sequences, quantity limits, or specialty-pharmacy requirements. These rules generally don’t exist in machine-readable formats [1][2].
As therapies have grown more complex, this gap has widened. Specialty medications, only 6.2% of prescriptions but 71.1% of spending, require the deepest review, the most variations across payers, and the most documentation [3]. The BV infrastructure simply wasn’t designed for this level of variability.
Workflow design compounds the problem. Benefit Verifications still require sequential, IVR/portal-based work, one case, one portal, one policy, one screenshot at a time. There is no way to orchestrate multi-source checks in parallel or automatically synthesize evidence across portals, PDFs, IVR calls, and policy documents. As volume increases, particularly for specialty drugs, throughput hits a natural ceiling.
Finally, BV outputs are still largely unstructured: screenshots, pasted notes, or free-text fields. Downstream teams, PA coordinators, pharmacies, providers, cannot rely on these outputs programmatically, which means every step after BV inherits the same manual burden. Without structured, auditable outputs, no downstream automation can be triggered reliably.
In short, BV fails today because the system was designed to move data, not to understand it. Eligibility became electronic, but the logic that determines access never followed. The industry now faces a structural problem, not a workflow problem, and solving it requires an entirely different foundation.
Closing the Gap
The challenges in BV persist because the underlying infrastructure cannot express or interpret benefit logic. Eligibility data moves electronically, but the information required to determine access, prior authorization criteria, step therapy, quantity limits, specialty-network rules, and site-of-care restrictions, remains locked in formats designed for humans, not systems, in particular IVR trees.
Neon Health approaches the problem by focusing on the underlying data model rather than the workflow. The system is built to do three things reliably:
1. Retrieve information from the sources where benefit logic actually lives.
This includes payer and PBM portals, policy documents, and electronic transactions. The goal is not to replace these sources but to read and extract from them consistently.
2. Interpret and normalize benefit rules into a structured format.
Coverage policies vary widely by payer and plan. Neon translates this variation into a uniform schema so that prior authorization requirements, quantity limits, and cost-share details can be evaluated consistently.
3. Produce a complete, evidence-linked verification record.
Every value captured, coverage status, access requirements, financial information, is stored alongside its source. This creates a verifiable BV artifact that downstream teams can use without rework.
Figure 4: Neon Health BV Acceleration Layer
This does not eliminate the complexity of benefit design, nor does it replace clinical or operational judgment. It simply removes the manual steps required to retrieve, interpret, and document the information that determines access. By treating BV as a data standardization and interpretation problem, rather than a portal-navigation task, Neon provides an infrastructure that can scale with the volume and variability of today’s therapies.
The result is not a different workflow, it is a more reliable foundation for the same decisions access teams make every day.
Sources
[2] CAQH Index 2024 – Full Report (PDF)
[4] MedCity News (2024): Managing the Specialty Drug Cost Challenge
Related articles
Related articles



Ready to transform Patient Access?
Ready to transform Patient Access?
NEWSLETTER
@ 2026 Neon Health (Belay, Inc).
AI-powered patient access automation
for leading pharma enterprises.
NEWSLETTER
@ 2026 Neon Health (Belay, Inc).
AI-powered patient access automation for leading pharma enterprises.
NEWSLETTER
@ 2026 Neon Health (Belay, Inc).
AI-powered patient access automation
for leading pharma enterprises.